Quick Links
Articles
| Why the need for IDPD? | |
| Beyond the Dyslexia Diagnosis | Amruta Veer |
| Make School Reopening Easy | |
| Stories | |
| Global Accessibility Awareness Day (GAAD) | |
| What is WAAD ? | |
| What is Purple Day ? | |
| Life is so beautiful, Just don't lose hope, overcome fear! | Shenaz Haveliwala |
| 'School teachers need to be educated about epilepsy' | |
| 50 Million Steps for Epilepsy | |
| What is UDID/स्वावलंबन UDID कार्ड | ChildRaise Team |
| World Cerebral Palsy Day | |
| The Learning Disabilities Awareness Month | |
| Light on Learning Disability | |
| Sibling Blessing | |
| Your Children are your Gift from God ! | Roopa Yennemadi Lobo |
| Marvelous Me ! | Chaya (Sheela) Ubhayakar |
| Need of Financial Planner | Mr. Jitendra P. Solanki |
| Developmental Milestones | |
| GADBAD | Dr. Manoj Bhatwadekar |
| What is D-Tour ? | |
| Maa - a Mother's Day Special | Divya Vinekar |
| Some Sunny Tips for Summer Vacation | |
| 'Trust your Gut' | |
| Acceptance is the magic 'Mantra' | Dr. Manoj Bhatawdekar |
| INDIAN NATIONAL ANTHEM IN INDIAN SIGN LANGUAGE |
|
A tribute to Shri. Kedarnath Udiyavar

There are some angels who are always present in your sphere in human form and when you are in need of utmost support, they spread their wings and engulf you in a warm hug. They are supremely humble and committed and do not seek recognition for all the good deeds they do.Their only purpose in life is to serve humanity, be compassionate and spread joy.
The ChildRaise Trust Team is extremely fortunate to have these angels in our lives so that we can continue our work in the field of empowering people with disabilities. With due respect, I cannot help but gratefully acknowledge and honour one of the most loving angels 'Vinati Udiyavar',who has extended great support to all our ChildRaise Projects; Be it development of www.childraise.com, Sanjivani project where we provide epilepsy medicines, therapy support to underprivileged children or the recent project of providing support for epilepsy brain surgery.
Shri. Kedarnath Udiyavar, Vinati's husband passed away suddenly on 26th October, 2020. On the occasion of Shri. Kedar's 5th remembrance, we would like to acknowledge dear Vinati's contribution to ChildRaise in his loving memory.
Shri.Kedarnath Udiyavar was the President & Business Head of OneMarkets at Intellect Design Arena Limited. His colleagues, associates, and students can go on speaking eulogies and writing lengthy tributes about his leadership, mentoring, and oratory skills.Such were his skill sets.But most important was how he balanced his professional, personal and spiritual life.
His colleagues have paid a tribute in a nutshell by expressing what Kedar meant to them .
K - Kind Hearted
E- Energetic
D- Dutiful
A- Affectionate &
R- Respected Leader
Any person who came in contact with Kedar could vouch that he was unique. He lived like a Yogi. A real Karmayogi. He supported many social causes. He initiated and nurtured Ullas - A CSR initiative by Polaris (now Intellect) working with students from Govt. schools focusing on their overall development emphasising "Can Do" spirit. Kedar knew that the wind beneath his wings was his wife Vinati, who with her silent yet strong support was always beside him. He was very proud of her deep involvement in women empowerment projects like Samvit Sudha & other social, religious, creative and charitable activities.Vinati says that she owes everything to him and he was the inspiration in her life.
We are honoured to keep Shri. Kedarnath Udiyavar's legacy alive and sentiment of giving back to society. We are sure that this support will illuminate so many lives.
Beyond the Dyslexia Diagnosis: Addressing Stigma, Stereotypes and Misconceptions

Every year October is observed as Dyslexia Awareness Month to raise awareness, enhance understanding of this condition provide the necessary support to these individuals and reduce stigma around it. For over 50 years, research on specific learning disabilities has been ongoing, providing us with ample reliable information and effective intervention strategies. Today, in most of schools, teachers, parents and school authorities are well aware of dyslexia and its academic implications. Despite this, stigma, stereotypes and misconceptions about this condition are rampant in our society. Such social implications of dyslexia adversely affect children’s socioemotional well-being even when they receive support to manage their academic challenges.
Over the past two decades, Dyslexia has gained increasing awareness in urban India. It is the most recognised form of Specific Learning Disability (SLD), characterised by difficulty in acquiring reading skills and spelling in children with normal vision and average intellect.
Today, when a child struggles with basic reading skills or consistently underperforms in school exams, concerns about dyslexia are quickly raised by both parents and teachers. The child is referred for assessments and if diagnosed with dyslexia, targeted interventions are planned and implemented. While these interventions focus on addressing learning challenges, they often overlook the emotional impact of the condition. The child's emotional well-being is frequently overshadowed by the emphasis on academic performance, leaving their inner struggles unnoticed. The stigma, stereotyping, and misconceptions associated with dyslexia can create a whirlwind of emotions for the child. As we observe this year’s Dyslexia Awareness Month, let us take the opportunity to examine these often-overlooked aspects of dyslexia interventions and gain a deeper understanding of the emotional world of children with dyslexia.
In order to address these social aspects around dyslexia, we need to understand what they exactly mean. ‘Stigma’ is a belief that arises when people are judged or treated unfairly because of something about them that others see as wrong or different. It makes people feel ashamed of their conditions and left out. When a child is diagnosed with dyslexia, she is often perceived differently both in the classroom and at home. Dyslexia is frequently seen as a deficiency or a more severe disability than it truly is. In school, children with dyslexia are often seated differently or ‘pulled out’ of the classroom for remedial sessions. These actions, though seem necessary, give rise to negative comments and labelling of these children. They are commonly called - ‘weak’, ‘unintelligent’ and ‘lazy’ due to their inability to perform in the classroom.
‘Stereotypes’ are oversimplified and fixed beliefs about a particular group of people based on a few characteristics. These generalisations assume that everyone in the group shares the same traits or behaviours, ignoring individual differences. We often hear statements like - ‘Children who cannot read fluently are lazy or not trying hard enough’, or ‘Children with dyslexia are less intelligent than other children in their class’, and ‘Children with dyslexia cannot succeed academically’. These statements group children with dyslexia into one broad category of academically underperforming students and as a result, their positive qualities and strengths are overlooked.
Specific Learning Disabilities can be complex to understand. With the explosion of information, it is difficult to differentiate factual information from incorrect ideas and beliefs. Misconceptions about dyslexia are rampant because of wrong assumptions and the spread of inaccurate information about its characteristics. For example, a common misconception is that people with dyslexia are not intelligent when in reality, dyslexia affects reading ability, not intelligence. Such misguided notions can result in parents and teachers dismissing the difficulties faced by these children.
Stigma, Stereotypes and misconceptions can seriously interfere with the child’s efforts to overcome her struggles in and outside of the classroom despite the diagnosis of dyslexia and interventions. When children are marked ‘different’ than their peers, it adversely affects their self-esteem. When parents and teachers view children with dyslexia through a lens of "deficiency" or "disability," they often unconsciously discriminate and lower their expectations of the child's achievements, especially in comparison to their peers at similar academic levels. This can also lead children to fear confirming these negative beliefs about themselves. When a child believes her shortcomings due to dyslexia to be their inherent weakness, it becomes a self-fulfilling prophecy where these beliefs gradually become her reality. Children are intuitive and observant. They understand other’s perceptions about them. As they internalise these perceptions, they may become a part of their identity. This may result in even poorer academic performance, lower sense of belonging and anxiety, which may continue well into adulthood.
As adults supporting children with dyslexia, it's crucial to understand the social challenges that come with the diagnosis. It is not a disease to be cured but a (different) way of thinking and learning. Being aware of these aspects helps us better maintain their self-confidence and motivation as they work to overcome their difficulties. Our focus should be on fostering their strengths while accommodating their limitations. For instance, teachers can arrange peer support activities to encourage active participation in the classroom. They can also design differentiated tasks and assessment methods that align with each child's abilities. For example, if a child struggles with reading fluently at grade level, providing simpler texts or assigning a peer to read aloud can be helpful. They should ensure these accommodations don’t lead to negative labelling or exclusion from the classroom. Even if parents and teachers are not fully trained in dyslexia interventions, they can still be mindful of the social impacts and create an environment where the child can thrive and reach her full potential.
Amruta Veer
Make School Re-opening Easy

June is the month of new beginnings and fresh starts. In India, the month of June usually opens with the first welcome showers of rain which helps to cleanse the body, mind & spirit of all dirt, lethargy and exhaustion. Everything appears new and fresh.
June is also the month of school re-openings. After a rather long vacation, the child eagerly waits for the school to begin as he is eager to show off his/her new pencil box, bag etc. and keen to reunite with friends or to make some new friends. However, with the new academic year, the child may face some new challenges, which could cause stress or anxiety.
There are numerous ways in which a parent can prepare the child for his/ her school reopening.
1) Plan a visit to the school before it opens officially;
2) Show the child his classroom, canteen or take a walk on the playground.
3) Plan his day as per his school timings a few days earlier.
4) Prior to school reopening, schedule his daily activities as per school schedule like his play
time,sleep times etc.
5) Motivate him with positive stories about school experiences.
Stories
Are you in search of creative, inspiring, engaging and educating stories which your children and students find relevant? We have found several stories and authors which can make your story time more fun and exciting!
A Hopi American Indian proverb says, “Those who tell stories
rule the world. Stories are a window to the world around us. They
are indispensable to early childhood education. They are a powerful
tool to put ideas into children’s world. They tell them how to think as
well as give them questions to think about. Storytelling is an
excellent way to lay facts. Stories are effective teaching and memory
aids.
As fascinating storytelling is, it is very challenging for both
teachers and parents. It is a struggle to recall an exciting and gripping
story when a child asks for it after completion of an academic task or
before going to bed.
While working as a teacher, previously I dreaded demand of a
fun yet meaningful story. I took help of story books available in the
school. But I found most of them irrelevant for my pre-teen students
with borderline intellectual capacity. These books contained not only
ideas and concepts more suitable in western scenarios but
vocabulary, which is cumbersome for our children, who do not have
English as their first language. It is difficult for our children to
understand terms such as autumn and turnips.
It is true that we already have most amusing, engaging and
insightful Indian stories which are still germane to our masses such
as Akbar- Birbal, Tenaliraman and our age-old favourite
Panchatantra. But as times change, we need new and as exciting,
stimulating, contextual Indian stories as the ones we grew up with.
Flipping through the story books laid on the school shelves, I
felt need of searching stories which today’s Indian children can relate
to and enjoy. I started my research and came across a number of
creative authors and vast array of stories which we all can rejoice. So,
every Saturday we will be posting one of our favourite stories,
information about authors and storybooks. Author Libba Bray says,
“There is no greater power on this earth than story.” Let’s harness
this power and help children write their own stories.
- Amruta Veer Shanbhag
Global Accessibility Awareness Day (GAAD)
.png)
May 16th is marked as Global Accessibility Awareness Day (GAAD) this year. Every year it is observed on the Third Thursday of May. Global Accessibility Awareness Day (GAAD) is an awareness Day focusing on Digital Access and Inclusion for the more than 1 billion people alive today who live with disabilities or impairments . GAAD was launched in 2012. It was inspired by a blog post by web developer Joe Devon who worked with Jennison Asuncion, an accessibility professional from Toronto , to co-found GAAD. This year it will be the 13th year of celebrating GAAD.
Why do we need to have GAAD?
The GAAD Foundation was set up in 2021 to mark GAAD's 10th anniversary. The purpose of GAAD Foundation is to initiate a conversation about what is meant by digital access and how to include more than one billion people with disabilities. Its mission is to ensure the technology and product development has Accessibility as its core requirement. Which in simple language means that the person with disability should have the same experience or opportunity to navigate the web space as successfully as the person without the disability. But in the current scenario, it is seen that the disabled community is underserved by today's digital products.
How does Inaccessibility affect people with disabilities?
People with blindness require alternative text descriptions. People who are deaf or are hard of hearing will need captioning or visual indicators. People with motor impairments may need alternative keyboards. And people with cognitive impairment may need uncluttered screens, simple language and consistent navigation.
People & the manufacturers of digital products have come to realise the importance of GAAD and are making a sincere effort to bring accessibility into digital experience and to include these more than 1 billion people with disabilities into the mainstream of society.
What is WAAD ?

WAAD is World Autism Awareness Day! WAAD is celebrated on April 2nd . It is celebrated to foster acceptance and understanding about autism. The theme for World Autism Awareness Day 2022 is ‘Inclusion in the Workplace’ & Inclusive education.Both are equally important and is the key to the transformative promise of the Sustainable Development Goals, to 'Leave no one behind'.This year‘s observance will address inclusive education in the context of SDG 4 - the promise and reality - through a virtual event that will include a moderated panel discussion, along with brief presentations by self-advocates, educators and other experts. The Event will take place on 8th April Time- 10 to 11.15 am EST -"Inclusive Quality Education for All " Registration is necessary. (For registration log on to www.un.org)
The theme of inclusive education is intrinsically linked with the focus of last year’s WAAD observance, “Inclusion in the Workplace”. Panelists in last year’s event emphasized how crucial it is to foster inclusive quality education for people on the autism spectrum so that they can fulfill their potential and achieve sustainable success in the labour market. In this respect, inclusive education is the key to the transformative promise of the Sustainable Development Goals, to LEAVE NO ONE BEHIND.
(Source- www.un.org)
Why the need to celebrate WAAD?
The statistics show that one in 66 children are affected by Autism & the numbers are rising so awareness is very important.
Epilepsy Article
What is Purple Day?
Purple Day for Epilepsy Awareness is celebrated on 26th March !
ChildRaise has been celebrating Purple Day for Epilepsy (Tendency to get Fits)since 2010. We really go all out to celebrate this day and make it a big event because there are very few organizations who focus on epilepsy in India. The statistics say that one person in every 100 has epilepsy.Though it is so prevalent, we still have so much stigma attached to it.
We are India partners with www.purpleday.org to spread epilepsy awareness & their message - "You are not alone & not to fear epilepsy". Cassidy Megan from Nova Scotia, Canada started her mission of Epilepsy Awareness at a very tender age in 2008. Her idea was very simple." Wear Purple & Show your Support to Epilepsy". Now recognised worldwide as a youth leader & an Epilepsy Advocate, Cassidy's initiative has spread to other parts of the world & has become a global event. Anita Kaufmann Foundation has joined her in this mission & taken epilepsy awareness on an international level. Their tagline is "Purple Day EveryDay". True to their words they are wonderfully creating awareness 365 days of the year.
Do log on to www.purpleday.org & www.purpledayeveryday.org to know more.
Life is so beautiful, Just don't lose hope, overcome fear! - Shenaz Haveliwala |

In 2005, at the age of 19, one week before my examinations, I lay down on my mother's lap complaining of a headache. The next thing I remember waswaking up in the hospital ICU. And, that was the first time I heard the word 'viral encephalitis'.
After mechanical engineering, I had decided to major in laser technology, a reality I had built in my head.I couldn't go back to university since I used to get seizures every day. Side effects of drugs were terrifying. My social life was hampered.
Mom and dad left nostone unturned. Everything they could do, was done. It was during this one year that i became part of the 'college editorial board' in the Times of India.I was still getting seizures almost every day. A miracle was my only hope.
Eventually I had to undergo a surgery atSreeChitra institute in Trivandrum. It was then that i came across patients from all walks of life; people from different cultures, age groups, cities, financial backgrounds. All of them bound by one common thread-epilepsy. It felt so relieving to know that I was not alone. There were millions battling with me. Unfortunately, for me, surgery was not a complete success. I have been on several AED's since the past nine years. I was desperate to support my medical expenses, at the same time, was fully aware that it will be difficult for me to find a job in another company. That is when, I decided to start a business of my own. I renovated my father's old warehouse in Fort to a conference hall. Since it is a commercial area, close to high court, there is a need for out of court settlements, arbitration matters etc. Giving it out on rent, I now support the finance of my own medicines. The hall is called SoboConnect and is now used for professional and other general meetings as well. It has made me feature inIndia's national business magazine 'Entrepreneur India'. Epilepsy could never stop me.
Promoting SoboConnect I learned the art of website designing. At the same time did not give up on my academics. Studying through correspondence, I graduated in the stream of commerce last year.
Currently, I'm working at the Indian Epilepsy Association (Mumbai Chapter) as a special educator for young adults with epilepsy. Along with regular studies, I strive to teach my students the importance of courage and persistence.In life, it does not matter how slowly you go, as long as you don't stop.
Just after I let happiness rule my life, in 2011, Dr. B.S.Singhal honored me with the'Most Courageously Living withEpilepsy' award. The same year, my story was featured in a book 'Conquering Epilepsy' edited by Carol D'souza.
I continue to get seizures and struggle to overcome the side effects of my current medication but i 'm happy I've learned to visualize the world my way. If you walk with hope in your heart, you never walk alone.
Few weeks ago, I received an award by the International Bureau of Epilepsy. I was invited to Singapore to receive a prestigious award at the Asian and Oceanic Epilepsy Conference as the 'Outstanding Person with Epilepsy'-2014. I encountered patients, delegates, doctors from various nations, cultures. It was overwhelming to see my work getting a global recognition.
My profession makes me so happy.It's now that I have become so much more grateful to Allah and can see the beauty in all his plans. Life will move forward, just keep in mind that there is light at the end of every tunnel.
For Epilepsy day this year, I will be inTrivandrum, to the same epilepsy ward I was admitted in for my surgery in 2007. Only difference is that this time, instead of being a patient I'll be going asthe guest of honor. Life is bringing me back to where I started from. It is such a proud feeling. Where there is a will, there is a way!
- Shenaz Haveliwala
'School teachers need to be educated about epilepsy' |
Many children suffering from epilepsy get little sympathy from their teachers when they get seizures in school and are often told to quit school, a health expert has said while underlining the urgent need to educate schoolsabout epilepsy and how to help affected students.
"I get many children who have been told by their schools to stay at home 'till they are cured'. This just shows the complete lack of understanding people have about epilepsy in India and how to manage this treatable health condition," said Mamta Bhushan Singh, assistant professor in the department of neurology at the All India Institute of Medical Sciences (AIIMS).
"There is a pressing need to organise talks in schools about epilepsy in order to educate teachers about it. If schools begin to stigmatize students affected by epilepsy as someone abnormal, then it increases the problem. It becomes more difficult for the child to cope. We need educators and counsellors besides doctors to help because epilepsy is a treatable disease," Singh said on the sidelines of a talk on 'Epilepsy: Need for greater awareness' at the India International Centre here.
The doctor's comments came after the mother of a child suffering from epilepsy said that her son was told by teachers of his well-known south Delhi private school to "remain at home till he is cured".
"This just shows the lack of awareness and understanding people have about epilepsy," the doctor said.
Around 10 million people in India - 10 out of 1,000 people - have epilepsy, but most do not have access to proper treatment, especially in rural areas.
"The treatment gap, which means epilepsy patients not getting treatment or getting inadequate treatment, is huge - around 70-90 percent. This is a dismal state of affairs," said Singh.
"There is a stigma attached to epilepsy, which makes people tend to keep it under wraps. This is wrong and harmful for the patient," she said, adding that many people run to quacks for treatment instead of coming to hospitals.
"Nowadays there are very good drugs to treat epilepsy, and in case the drugs do not work surgery is also done in special cases, which has proved very beneficial," Singh said. AIIMS is one of the few hospitals in India where specialised surgery is done for epilepsy patients.
Asked if ayurveda is helpful in treating epilepsy patients, Singh recounted the case of a well-known "ayurveda" doctor in Haridwar who would put out huge advertisements in newspapers of how he could cure epilepsy with his "wonder herbal drug".
"We at AIIMS were worried because many of his patients began to report to us," she said. The quack was arrested and when his "herbal medicine" was examined at AIIMS they found it to contain a mixture of 3-4 known allopathic epilepsy medicines.
"He would crush the allopathic medicines into a paste and administer it to epilepsy patients, irrespective of their symptoms or severity. This was even more dangerous."
A major reason for children getting epilepsy is head injuries. Children fall off open roofs, which don't have ramparts, during play and hurt their heads, which results in scarring of the brain.
Babies born at home are at risk of getting epilepsy, she said. "The baby born at home could cry late and there would be no doctor to provide immediate treatment, this could lead to epilepsy. A difficulty in birth could also result in the baby developing epilepsy," Singh said.
Another major contributor to epilepsy cases is eating unwashed leafy greens. Green vegetables like cabbage and lettuce, which grow near the soil surface, could have tapeworm eggs. These eggs if ingested travel through the blood stream to the brain and cause epilepsy seizures.
Singh said eating leafy green vegetables served in hotels, especially those in sandwiches and in Chinese dishes, which are partially cooked, should be avoided.
These are causes for epilepsy that are "preventable", said the doctor.
Don't pin down a person getting an epilepsy attack, just make him/her lie down on one side and remove any sharp objects from near the person. Don't also try to put something in their mouth, she added.
Source - www.indiaedunews.net
50 Million Steps for Epilepsy
50 million people worldwide are affected by epilepsy according to WHO/OMS official figures.
For many people living with epilepsy, the stigma attached to the disease is more difficult to deal with than the disease itself.
To raise awareness and to raise vital funds for epilepsy organisations across the world,
the International Bureau for Epilepsy (IBE)
is asking people to join together to walk 50 million steps in the lead up to International Epilepsy Day –
one for each person in the world who has epilepsy – as part of the ‘50 Million Steps for Epilepsy’ challenge.
Do Join Us in this Campaign.
Click on this link to know more-
https://www.ibe-epilepsy.org/50millionsteps/
What is UDID |
The full form of UDID is Unique Disability ID. Unique Disability ID Card (UDID Card) is being issued to all the disabled persons who register for it. This card is also known as Swavlamban Card and it comes with a number of benefits.This UDID project is initiated by the Department of Empowerment of Persons with Disabilities which aims at building a holistic end-to-end integrated system for Issuance of Universal ID & Disability Certificates for Persons with Disabilities with their identification and disability details.
PwDs are required to register with the UDID portal. Once registered, after the login is complete, they will be able to apply online for a Disability Certificate and UDID card. How to register for the UDID and to know about the description of the workflow click on http://www.swavlambancard.gov.in/
A person with less than 40% disability would have a card with a white stripe, 40 to 80% would have a card with yellow stripe and above 80% card with a blue stripe. A unique 18-digit number would be given on the card, which would have state identification digits, district code, disability code, year of birth and another sequence.
Read more at:
https://economictimes.indiatimes.com/news/politics-and-nation/colour-coded-cards-to-be-launched-for-2-7-crore-disabled/articleshow/55929479.cms?utm_source=contentofinterest&utm_medium=text&utm_campaign=cppst
https://www.indiatoday.in/information/story/how-to-apply-online-for-udid-card-a-complete-guide-1618567-2019-11-13
https://economictimes.indiatimes.com/news/politics-and-nation/colour-coded-cards-to-be-launched-for-2-7-crore-disabled/articleshow/55929479.cms
To know more (In Hindi) https://www.youtube.com/watch?v=sQoDgc7OjYc
World Cerebral Palsy Day |
Know more about Cerebral Palsy, the most common childhood disability.Why there is a need for World CP Day?
World Cerebral Palsy Day will be celebrated all over the globe on October 6th. What is World CP Day & why it is celebrated?
Cerebral Palsy is a complex condition and can pose a lifelong disability.It mainly affects movement but affected persons can have visual, hearing, speech and intellectual impairments. Nearly 70% of children with CP have epilepsy. CP can be mild to severe.
It is celebrated to create more awareness of the condition as a person with CP can evoke a wide range of emotions from sympathy, pity to neglect, rejection and isolation.
The colour for CP campaign is chosen as Green to represent youthfulness, new growth and also hope for advancements in treatment and acceptance.
We need to celebrate the achievements of people with CP so more & more people become aware and we inch towards an inclusive society.
Read more on Cerebral Palsy
https://www.childraise.com/CP_Warriors.html
https://www.childraise.com/c_palsy.html
October – The Learning Disabilities Awareness Month |
The open house at my school are one of the most difficult days at work. Here, by ‘my school’ I mean the school where I work as a part-time remedial teacher. On one such open house day, while I was explaining one of my student’s report card to her mother, she was accompanied by a relative. The relative was listening to our conversation closely. After we were done, she casually asked, “Do you get a lot of ‘naughty’ children like this one here?” I just smiled.
In school, I work with children who cannot perform academically at par with their grade levels. To put crudely, the ones who cannot read properly, make frequent spelling mistakes, do not take interest in studies, cannot copy from the board, disturb the class amidst an activity – the ‘naughty’ ones. They are categorized by the school as ‘LD children’- worry for the school, burden of the teachers and puzzles for the parents. These are children with Specific Learning Disability, mostly Dyslexia.
Google says, Learning disabilities are a groupof neurological conditions which involve difficulty in learning to read or interpret words, letters, and other symbols or/and write or basic arithmetic operations withoutaffecting general intelligence. There are two takeaways here – neurological condition and general intelligence. As it is a neurological condition, it is life-long and cannot be treated. Learning disabilities are seen in children and adults with average or above-average intelligence. The definition itself says that people with LDs are intelligent, then why are they labelled ‘stupid’? Our education system is gnarled with the pen and paper method so much that these children who cannot work their way around it, are considered disabled or at disadvantage.
It is true that reading and writing are indispensable academic skills. They are essential in any kind of education system. Students with dyslexia can achieve them with therapeutic learning methods. A number of students with learning disabilities pass their exams with flying colours once they learn to manage their condition. Special education courses comprehensively cover different symptoms of LDs , their management, effective teaching methods and provisions provided to these children. We are taught to focus on what they cannot do and how we can remediate that, but we are never taught what they can do? If their brains are wired differently, what they have to offer?
40% of self-made billionaires are dyslexic. What about Leonardo da Vinci, Albert Einstein, Walt Disney, Richard Branson or even Tom Cruise! How did they do all that with Dyslexia?
For years Dyslexia or any other learning disabilities are viewed as limitations or incapacities. This Learning disabilities awareness month let us try to view the children with learning disabilities in different light and let them shine in their own way!
- Amruta Veer
Amruta is a Remedial Teacher. She works as a freelance remedial teacher in a mainstream school and provides remedial services at ChildRaise Centre.
She holds inclusive workshops for kids with special needs and others at ChildRaise Centre. She also writes for www.childraise.com
Light on Learning Disability |
Poems are the best way to express emotions and feelings, in a nutshell.
These two heartfelt poems on Learning Disability or Difficulty (LD)
explain the condition without the barrier of definitions, terms, and jargon.
These poems speak of hope, understanding, and triumph of the human spirit.
Sibling Blessing |
Meet a new emerging generation of siblings who are a blessing to their parents and their brother, sister with special needs. Know more about what role they play in this special journey!
Siblings Day is a holiday recognized annually in some parts of the United States and Canada on April 10, and as Brothers and Sisters Day on May 31 in Europe, honouring the relationships of siblings. Undoubtedly, this is a unique bond but when the sibling is a brother or sister with special needs, it becomes a little complicated one.
Parents are often worried when they have a child with special needs. And usually the responsibility of looking after the adult with special needs is handed over to the sibling whether they feel involved in the care of their sibling or not. Often, parents think of admitting their child in life care centres because they do not want their other children to bear the care of their sibling.
But now, the times are changing. Gone are the days when parents were guilt ridden because they felt they were doing injustice or demanding much more from their other children to take care of their brother or sister with special needs. The new breed of siblings are coming to the forefront and playing active roles in their sibling’s lives.
Welcome to the world of sensitive, sensible, caring human beings who are blessings in the form of siblings. They have understood that their brother or sister with special needs is an occurrence of no fault of their parents or them.
Get to know some of the inspiring siblings who have made a difference not only in their siblings lives but in the lives of others who are travelling on the same path.
Reach Out
In any programme dealing with disability if you come across a cheerful smiling lady along with a smiling adult in his fifties, this duo is sure to be Rekha Balgi & her brother Girish Balgi who is mentally challenged. Rekha is a special educator, trained counsellor & a Yoga instructor. She is the Founder of Reach Out which was formed in 1997 that organises activities to create Inclusion & Awareness. Recently she has published Reach Out- Make a Difference guide which addresses issues like financial security , what after us which constantly cloud the minds of the carers of people with special needs.
Nayi Disha
Prachi Deo’ s brother who has Down’s Syndrome is her inspiration in setting up Nayi Disha. This is an information resource for intellectual and Developmental Disabilities (IDD). She quit her job in the software sector to pursue her passion for working on the issue of IDD.
Check out www.nayi-disha.org
Reservoir
Shreya Jain set up Reservoir because she has a brother with autism and fully understands the struggles of families. Her organisation helps parents and caregivers navigate the legal framework and set up trust funds, letters of intent and UDID for children with special needs. . Reservoir’s online platform, which was launched last year, takes care of two other core objectives: curating resources for caregivers and building a network of trusted professionals for therapy and other needs.
Read more on www.reservoirnow.com
Veruschka Foundation
Late Veruschka Dias and Late Mariamma Thomas were beacons of joy and life, who surpassed their developmental disabilities to inspire two young women – sister Tatyana Dias, a neurbiologist and niece – Christina Joseph, a financial professional respectively to help other individuals like them find a voice and place in our society. They set up Veruschka Foundation to realise their dream of an inclusive society that Accepts, Celebrates and Empowers differently-abled individuals.
Read more on - https://theveruschkafoundation.org
Saarthi (meaning Charioteer)
Sibling Support Network India is a community of siblings of persons with intellectual & developmental disabilities and other disabilities.
Awesome Heroes with Autism |
Presenting stories of Varun Sawant & Kabir Kumta. They have autism. Meet them and feel inspired.
Varun Sawant's resolve to go beyond the finish line was path-breaking. Procam International has released a wonderful video on him
on World Autism Awareness Day, describing his journey towards becoming Asia's first marathoner with Autism!
Click to view
Kabir Kumta - Flower Power and the power of Autism
Kabir has autism. He loves meeting people and experiencing new places. Making torans and haars and
hand-delivering them to his customers allows him to
be a part of the fun and festivity for which the torans and haars are ordered.
Kabir’s Kreations have adorned homes, workplaces, exhibitions in colleges ...
with each delivery Kabir has received much more than his fee.
There has always been heartfelt appreciation, sometimes accompanied by a hot cup of tea ...
and occasionally a box of kaju kaatri or hot khaman dhokla ...
Some of these he loves and some he tries with some apprehension.
All in all, Kabir’s Kreations opens up the world to Kabir and Kabir to the world :)
Visit his Facebook page- https://www.facebook.com/Kabirs-Kreations
and meet other awesome heroes with Autism.
Peace With Pace
A Child, Wonderful gift from nature.
My Child, my link with the future.
When my child smiles, my world shines.
When my child cries, a part of me dies.
I wish to teach my child to the best of my ability,
But.. I am shocked to discover, he has a Learning Difficulty!
My child fumble with alphabets, letters.
His study time give me jitters.
Oh my child.. all these letters lead to a treasure,
How can you be deprived of this divine pleasure.
I know my child, Learning is difficult game for you.
Even writing your name is a great achievement for you.
I will wait my child, for the Golden day,
Till you find your Pace, Then I will attain my Peace!!
- Kavita Shanbhag
"I CAN" poem is the outcome of all the observation, experiences and chats Jagriti had with me during my PGDSE course. More I used to tell her, more she used to probe. She started developing empathy towards her classmates who suffer with their academics. She understood that the dumb and stupid are the meaningless words as there is a reason for every behaviour. She was so happy to know that her mom is trying to understand them and help them. She was motivated to pour herself on the paper. This poem is what she knows and experienced, with her mom in this beautiful journey of special education.
- Geeta Singh
I CAN
I am the child that looks healthy and fine.
But something is different, somewhere in my mind,
I want to learn, I want to know
But with different method and different goals
Every day I try my best
But I always get the lowest my test
I am not lazy, I am not smart
It’s just my mind, doesn’t seem to know where to smart
Don’t tell me what the world knows
Tell me that I don’t know
I just need your attention sometimes
Even you know that, deep inside.
Sometimes when I run around the class messy
You think that I’ve gone crazy
But hear me out I’m just a child
Like all the other children you can’t expect me to walk a mile
So what I’m asking is just for your help
To make me batter, to make me feel like everyone else
So, I don’t have to go home every day and cry
And think that my whole life has been a lie
It only takes one compliment to make me feel better
I hope you understand that by reading this letter
I CAN be like you, her, and him
All need, is you to understand who I truly am.
- Jagriti Singh
Your Children are your Gift from God !- Roopa Yennemadi Lobo |
When I held Rewa for the first time I knew I had a tough role to play, but didn't really gauge the intensity of it . She had delayed milestones but was coping fairly well, I first discovered her block when she began studying hindi in class 3, she would write A for K and K for A consistently. At first I ignored it and like a typical mother and educator verbally lashed out at her. 5 months down the line I knew that there was something drastically wrong somewhere, I approached an education and counseling centre Drishti and her diagnosis said it was LD (Dyslexia, Dysgraphia and Dyscalculia).
I was like any other parent upset at first but the educator in me took over quickly, I knew this was her and my battle for life and if I would not have handled it well then she would never learn to cope. I first approached her school Gundecha Education Academy at Thakur Village Kandivali East. Now time to say hats off , the school has an excellent plan for Special children and they took over her disability beautifully. From Rajashree Pawar her first special educator, to her major pillar of strength Padmaja Sabnis , support came in waves. Her concessions, her special education sessions were so beautifully given and conducted. They not only equipped her to deal with her disability but encouraged her creativity at school, She is excellent at drawing and photography and has bagged several prizes for both. that I can't thank them enough, Yes one word would say it all "grateful". I would also go on to say that Purnima Sharma her private tutor and special educator would come in line after me for the pains she has taken to shape Rewa.
I knew that my role as a parent would be ongoing. From running to get her tests done at Government hospitals to dealing with her feeling of hopelessness, I saw a new me emerging, a spirited and a strong minded me who had to wake up every day and tell my child "it's our battle and we need to fight it out".
As readers I would like to tell you this, always be an advocate for your child, be a very proactive parent and seek help for your child. Also become your own expert. Keep up with the new developments in learning disability programs, therapies, and educational techniques but don't forget you are the expert and the biggest influence for your child when it comes to finding the tools he or she needs in order to learn. Always stay positive and do not make the child's disability the center of their and your life. Remember your support encouragement and positivity will have a lasting impact on the child. At the same time understand that you have a life too do not over invest in the disability so much that you have no life of your own, go out into the world and do what you want, take care of yourself and take help wherever and whenever necessary. Let your family and friends know about your child's disability and the way you are dealing and coping with it.
Broadly think of life's success rather than just academic success and enjoy life with your child. Life itself is a teacher and trust me, your children will do as good as any other child with your ongoing love faith and trust in them!

What Roopa says about herself.....After 1 year at Lady Engineer High School, 11 years at Carmelite Convent English High School (old schools of thought) and 10 years at Kangaroo Kids Education Ltd (modern school of thought) .... Finally creating my own world of leading a team of 32 live wire teachers at N.L.Dalmia High School Pre Primary Section....A golden lesson I learnt in these 22 years in the field of education."The agony and the ecstasy of the parents rich or poor, parents of kids having special needs or not, is just the same!!"
Marvelous Me ! |
Chaya (Sheela) Ubhayakar.. a committed Teacher writes about her experience of being a teacher of a Marvelous Student. What does she have to say about this marvelous student?
"You have enriched my life like no other last year
And, are growing more marvelous each day this year.
My heart swells when I glimpse you in the hallways
When you shyly smile and say "I miss you" always
I miss you too, my dear and your presence in my class
But, you must move on and on and I have to stay, alas"
Being a sensitive teacher she knows what is going on in his mind & she has given words to his thoughts...

Marvelous Me !
I live in a wonderful world all of my own
I see things that you may not see.
I have feelings that you may not have.
You may see me as different, not like you
Remember, I am just marvelous ME !
I don't take to changes certainly
I don't like show of affection
I don't display much emotion
I get overwhelmed easily
Remember, I am just marvelous ME !
Please don't talk around or over me
Because I don't converse like you do
Simple events may set me off quick
That doesn't mean I am idiotic
Remember, I am just marvelous ME !
I am much smarter than some
Contrary to your assumption
In fact, I learn things faster
Complete my assignments quicker
Remember, I am just marvelous ME !
So, take some time, be patient
You may not get to know me
Or this wonderful world of mine
I have a label, called "Autistic", but,
Remember, I am just Marvelous ME !
Ms. Chaya Sheela Ubhayakar, a retired teacher wonders how her students with Autism must be coping in this Corona Pandemic.
She expresses her concern and sends love through her open letter.
I often wonder how you are faring
Now, that times are so confusing
Gone is your favored life of routine
Riddled daily with changes umpteen
School closed, lessons taught on line
Dad, mom, siblings home all the time
What happened suddenly, so peculiar?
Everything looks the same yet unfamiliar
Am sure you are trying to understand
Make sense of this situation, a bind
Wish your parents, you, I could meet
Help your fears, confusion, to alleviate
Alas, we have to keep distance now
But, my wishes will reach you somehow
Stay safe, healthy, take care, my dear
Sending hugs, love, good vibes, prayer
Ms. U ❤️
April 2020

Presently teaching Math and Science to 3rd grade students in a wonderfully diverse school in Houston , Texas, USA, Chhaya (Sheela)Ubhayakar graduated from Elphinstone College, Mumbai, India and University of Houston Downtown, Texas USA. She is certified in General, Special & Gifted/Talented Education. She loves to read, write, art, craft, act and cook. She enjoys being with family & friends. Sheela says ..."I am Passionate about my work, especially teaching and learning from challenging students."
Developmental Milestones |
Here is a chart which will give you the guideline when a parent feels there is something amiss with their child. One can always refer to these Developmental Milestones to know whether your child is progressing or lagging behind.
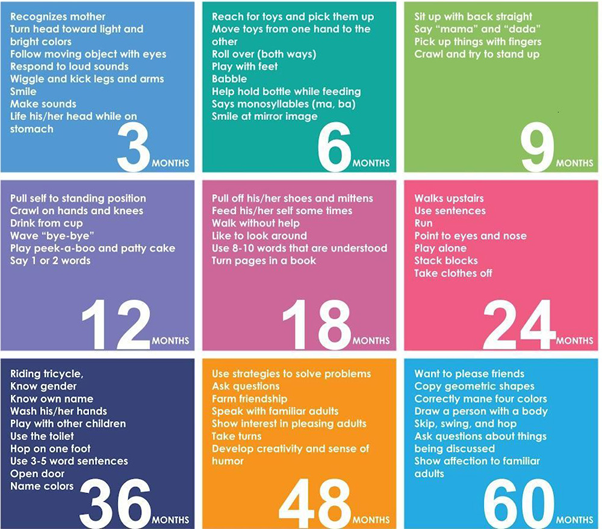
As soon as you detect any abnormality or have any doubts, take your child for diagnosis, treatment, and management to:
| Family Physician | Initial / Preliminary Diagnosis |
| Pediatrician | Initial / Preliminary Diagnosis |
| Developmental Pediatrician | Conclusive Diagnosis |
| Neurologist | Cerebral Palsy, Intellectual Disability, Epilepsy, Learning Disability |
| Clinical Psychologist | Intellectual Disability, Autism, Learning Disability, Epilepsy |
| ENT/Speech Audio Therapist | Hearing Impairment, Cerebral Palsy, Intellectual Disability, Learning Disability |
| Eye Surgeon | Visual Impairments, Cerebral Palsy, Learning Disability |
| Physiotherapist / Occupational therapist | Orthographically Handicapped, Cerebral Palsy, Learning Disability |
| Orthopedic Surgeon | Orthographically Handicapped, Cerebral Palsy |
| Remedial / Resource Teacher / Special Educationist | Learning difficulty, Intellectual Disability, Cerebral Palsy |
| Psychiatrist | Emotional/Behavioral problems, Attention Deficit Hyperactivity Disorder (ADHD) |
| Counselors | Emotional / Behavioral problems |
| School teachers | Detection of scholastic problems and implementation of an educational plan |
| Child Guidance Clinics | Assessments & Holistic Management |
'Trust your Gut' |
Often parents of special children have reported that they always knew
there was something wrong with their child. Even professionals believe
that gut feelings or parental instincts are never to be ignored.
So do not neglect your gut feelings and always act upon your instinct.
Once you have any reason for doubt about your child's development
depending upon the problem or condition, you should take your child
for diagnosis, further treatment and management to:
1 Family Physician Initial / Preliminary Diagnosis
2 Pediatrician/
Developmental Pediatrician Preliminary Diagnosis
Confirmation of Diagnosis
3 Neurologist Neurological defects like CP MR, Epilepsy, etc
4 Clinical Psychologist MR, Autism, Learning difficulty
5 ENT/Speech audio therapist Hearing impairment,CP
6 Eye surgeon Visual impairments, CP, Learning difficulty
7 Physiotherapist / Occupational therapist Orthopaedically Handicapped ,CP
8 Orthopedic surgeon CP, Orthopaedically handicapped
9 Remedial / resource /special educationist Learning difficulty, MR, CP
10 Psychiatrist Emotional/Behavioral problems
11 Counselors Emotional/Behavioural problems
12 School teachers Detection of scholastic problems and
implementation of educational plan
13 Child Guidance Clinics Holistic management
Do not indulge in doctor shopping but see to it that your doubts are
cleared and you give the best to your child!
Acceptance is the magic 'Mantra' |
The parents go through a spectrum of emotions once they realise that
their child is different than the rest. Dr.Manoj Bhatawdekar, a
leading Mumbai psychiatrist aptly describes the parental emotional
state in a nutshell. He calls it as "GADBAD".-----Read More
In read more-Know about GADBAD & be reassured that you are not the
only one who feels these extreme emotions. Every special parent goes
through GADBAD and how to overcome it.
What is GADBAD
Guilt - The parents feel guilty about giving birth to such a child.
They think-'I must have done some mistake in the past, that's why my
child has developed this disability".
Anxiety - They are constantly anxious. They worry about the future.
Denial - The parents do not accept the diagnosis. they feel it must be wrong.
Bargain - Parents try to bargain. e.g. can I stop the medication for my
child or can I give medicine just once instead of twice/thrice?. Same
happens with therapy sessions also.
Anger - The parent may express anger towards his/her child who has
disability or towards spouse, family members, the doctor or entire
medical system/society.
Depression - Parent expresses sadness, helplessness and negative
attitude regarding the possible outcome of disability.
Parents who have overcome the GADBAD stage, recommend the magic mantra
of Acceptance & vouch that this is the only way which will lead to the
road of recovery.
Celebrate Indepence Day


{kind=link}